

Explore how Transitional Care Management (TCM) works, why it matters, and how it reduces readmissions while improving care continuity.
Transitions between care settings, such as from hospital to home or a skilled nursing facility, are among the most vulnerable moments in a patient’s healthcare journey. Without proper coordination, patients may experience medication errors, missed follow-ups, or worsening symptoms that lead to hospital readmissions.
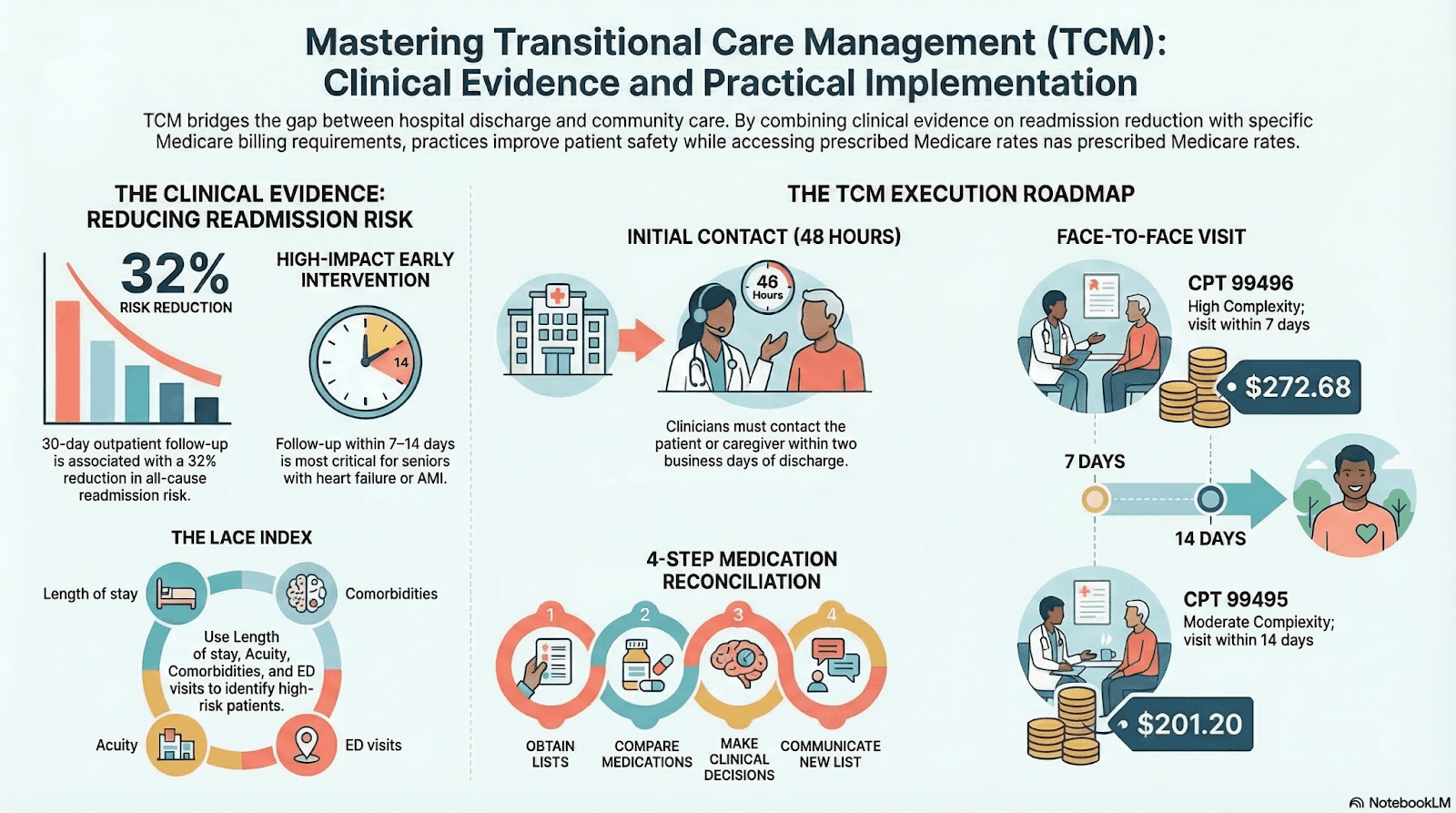
Transitional Care Management (TCM) programs are designed to bridge this gap. They ensure that patients receive structured follow-up, care coordination, and support during the critical weeks after hospital discharge.
Typical TCM services include:
- Post-discharge patient outreach
- Medication reconciliation
- Coordination with primary care and specialists
- Monitoring for complications or symptom escalation
- Scheduling and managing follow-up visits
By addressing care gaps early, TCM programs improve outcomes while reducing avoidable hospital utilization.
Why Care Transitions Are High-Risk
The period immediately after hospital discharge presents several challenges for both patients and providers. Care plans often change quickly, and patients must manage complex instructions without direct clinical supervision.
Common transition-related risks include:
- Medication confusion: Changes in prescriptions can lead to errors or missed doses.
- Lack of follow-up care: Patients may delay or miss essential follow-up appointments.
- Incomplete discharge understanding: Patients may not fully understand care instructions.
- Limited communication across providers: Information gaps between hospitals, primary care providers, and SNFs can disrupt care continuity.
These issues contribute significantly to hospital readmissions and emergency department visits.
Core Components of Transitional Care Management Programs
Effective TCM programs follow structured workflows designed to maintain close oversight during the post-discharge period.
Timely Post-Discharge Patient Contact
Initial outreach helps identify patient needs and clarify discharge instructions.
- Follow-up communication: Patients are contacted within a few days of discharge.
- Care plan review: Staff confirms the patient understands medications and treatment instructions.
- Risk identification: Early symptoms or concerns are flagged for provider review.
Medication Reconciliation
Medication discrepancies are one of the most common causes of complications after discharge.
- Review of discharge medications: Care teams compare hospital prescriptions with previous medication lists.
- Identification of conflicts: Duplicate or conflicting prescriptions are resolved.
- Patient education: Patients receive guidance on correct medication usage.
Care Coordination Across Providers
TCM ensures that all providers involved in the patient’s care remain informed and aligned.
- Communication with primary care physicians
- Coordination with specialists or SNFs
- Transfer of discharge documentation and treatment plans
Strong coordination reduces gaps that often lead to treatment delays or duplication.
Scheduling and Managing Follow-Up Visits
Timely follow-up appointments are essential for evaluating recovery progress.
- Appointment scheduling: Visits with primary care providers or specialists are arranged soon after discharge.
- Monitoring recovery progress: Providers assess symptoms and adjust treatment plans.
- Escalation when necessary: Patients showing complications can receive immediate clinical attention.
Significance of Transitional Care Management for Health Systems and SNFs
For healthcare organizations, TCM programs provide both clinical and operational benefits.
Reduced Hospital Readmissions
Consistent follow-up during the post-discharge period helps prevent complications that would otherwise lead to rehospitalization.
- Early symptom detection
- Timely treatment adjustments
- Better adherence to care plans
Improved Care Continuity
TCM strengthens coordination across healthcare settings.
- Hospitals, SNFs, and outpatient providers share patient information more effectively.
- Care plans remain consistent across transitions.
- Providers gain better visibility into patient recovery progress.
Better Patient Experience
Patients often feel overwhelmed after leaving the hospital. TCM programs provide reassurance and structured support.
- Patients have a point of contact for questions.
- Care instructions become clearer and easier to follow.
- Ongoing communication increases confidence in recovery.
Stronger Performance in Value-Based Care Models
Reducing avoidable hospital utilization is a key priority for organizations participating in value-based reimbursement programs.
TCM helps support these goals by:
- Preventing unnecessary readmissions
- Improving care coordination metrics
- Strengthening chronic care follow-up
The Growing Importance of Structured Care Transition Programs
As healthcare systems move toward more integrated and value-based care models, effective transition management is becoming increasingly important.
Hospitals and SNFs that implement structured TCM programs can better manage high-risk patients, improve outcomes, and maintain continuity of care across settings. These programs also help organizations address operational challenges associated with patient handoffs and post-discharge care management.
Many healthcare organizations now complement internal care teams with specialized platforms and care management support that streamline patient outreach, documentation, and coordination workflows.
Solutions such as Circle Health Care, for example, help providers operationalize transitional care programs by supporting patient follow-ups, care coordination, and structured monitoring during the post-discharge period.
Conclusion
Transitions between care settings represent a critical moment in the healthcare journey. Without proper oversight, patients are vulnerable to complications, medication errors, and missed follow-up care.
Transitional Care Management programs help close these gaps by providing structured support, proactive outreach, and coordinated care during the weeks following hospital discharge. For SNFs and health systems, effective TCM programs improve patient outcomes while strengthening care continuity across the healthcare ecosystem.