

Discover how Skilled Nursing Facilities (SNFs) can reduce 30-day hospital readmissions, improve CMS star ratings, and strengthen financial performance through structured transitional care, proactive monitoring, and coordinated care programs.
For Skilled Nursing Facilities (SNFs), reducing hospital readmissions is not just a clinical priority — it is an economic imperative.
In today’s value-based care environment, 30-day rehospitalizations influence:
- CMS Five-Star Quality Ratings
- Skilled Nursing Facility Value-Based Purchasing (SNF VBP) performance
- Hospital referral relationships
- Census stability
- Long-term revenue predictability
For SNF leaders focused on financial performance, improving readmission metrics is one of the highest-return operational strategies available.
This guide explains how SNFs can reduce readmissions, protect ratings, and strengthen economic performance, without adding operational strain.
Why Readmission Reduction Is a Financial Strategy
Hospital readmissions don’t just affect clinical outcomes; they directly influence how your facility is rated, reimbursed, and perceived by referral partners. In a value-based care environment, preventing avoidable rehospitalizations protects both performance metrics and long-term financial stability. For SNF leaders, readmission reduction is a strategic lever for sustainable growth.
1. Star Ratings Directly Influence Referrals
CMS star ratings are publicly reported and heavily scrutinized by:
- Hospital discharge planners
- Accountable Care Organizations (ACOs)
- Managed care organizations
- Families evaluating post-acute options
A lower rehospitalization rate contributes to stronger quality scores, which:
- Improves referral volume
- Protects occupancy
- Differentiates your facility in competitive markets
In many regions, even a half-star improvement can materially impact the census.
2. SNF Value-Based Purchasing (VBP) Adjustments
Under the SNF VBP program, Medicare adjusts payments based on hospital readmission performance. Facilities with higher-than-expected readmissions face reduced reimbursement, while strong performers can earn incentive payments.
Reducing preventable transfers, therefore:
- Protects the base Medicare revenue
- Minimizes downside risk
- Positions your facility for performance-based gains
For economically focused administrators, this is not simply quality improvement — it is margin protection.
3. Hospital Alignment in a Value-Based Ecosystem
Hospitals increasingly evaluate SNFs based on:
- 30-day readmission rates
- Transitional care reliability
- Medication reconciliation processes
- Communication responsiveness
Preferred SNF networks are built around measurable outcomes. Facilities that demonstrate structured readmission-reduction programs are more likely to secure consistent discharge flow.
The Operational Drivers Behind SNF Readmissions
Most avoidable rehospitalizations stem from breakdowns in transitional workflows rather than inadequate bedside care.
Common gaps include:
- Delayed follow-up after discharge
- Incomplete medication reconciliation
- Poor visibility into early clinical deterioration
- Fragmented communication between care teams
- Limited monitoring for high-risk chronic conditions
- Lack of structured 30-day transition tracking
The highest-risk period is the first 7–14 days post-discharge — yet many facilities lack standardized workflows for that window.
Reducing readmissions requires a system, not isolated interventions.
6 Core Strategies SNFs Use to Reduce Readmissions
Reducing readmissions requires more than isolated clinical improvements; it demands structured, repeatable systems. High-performing Skilled Nursing Facilities focus on coordinated workflows, proactive monitoring, and disciplined follow-up processes. The strategies below form the operational foundation for sustained reductions in 30-day hospitalizations.
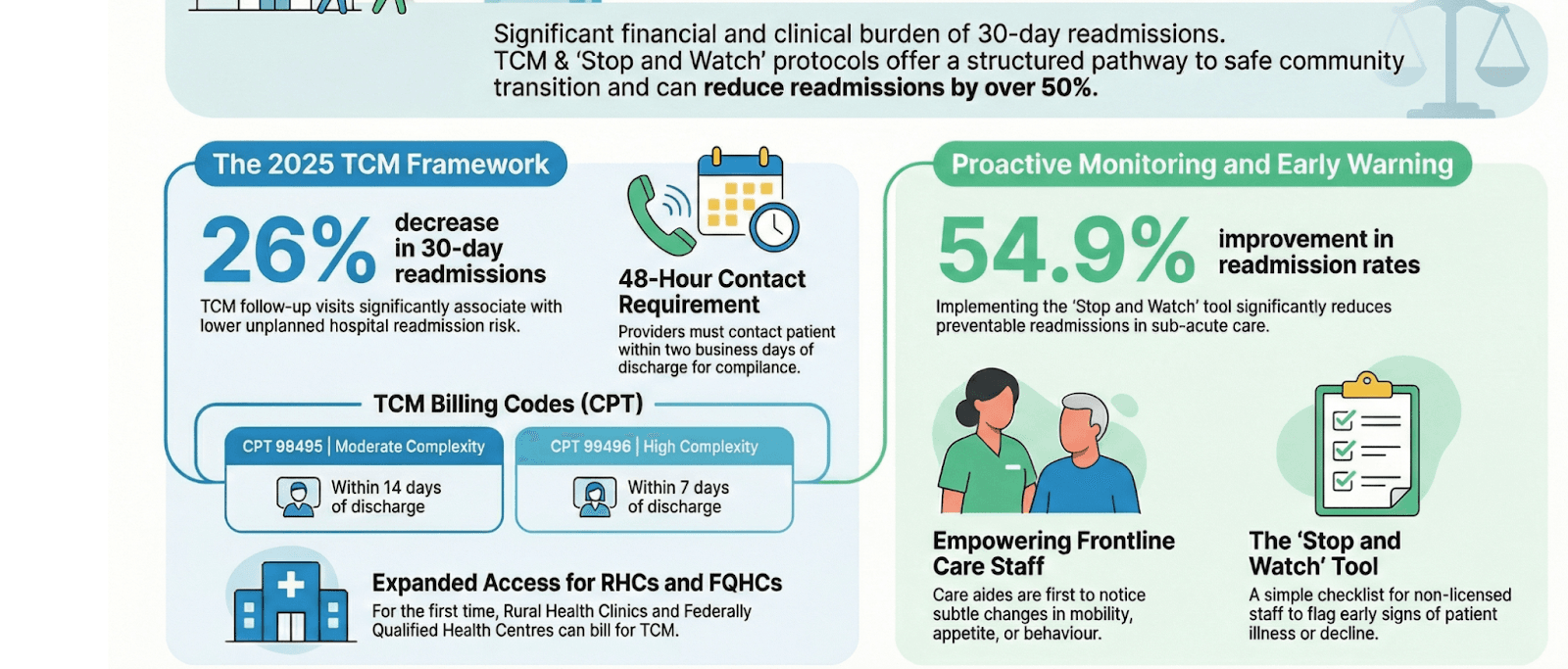
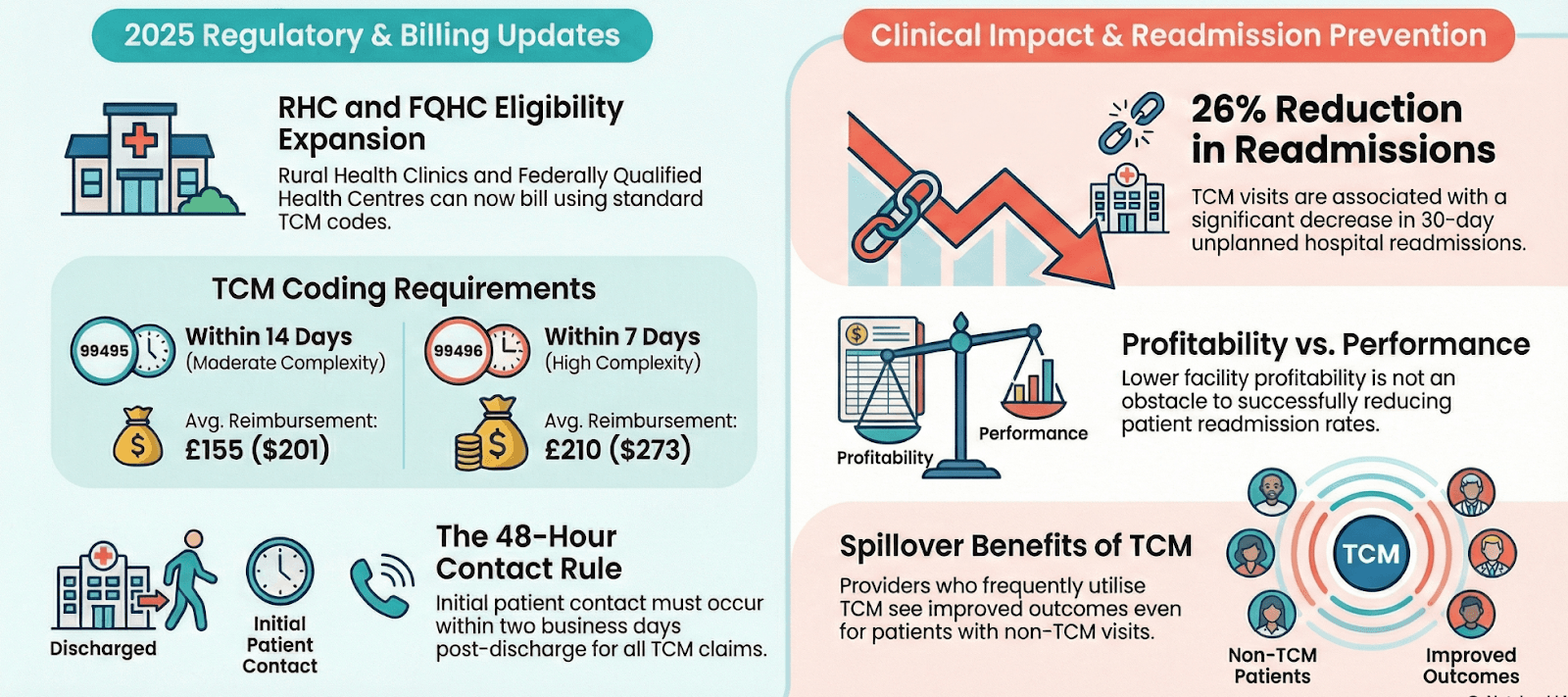
1. Implement Structured Transitional Care Management (TCM)
The 30-day post-discharge window is where economic performance is won or lost.
A structured Transitional Care Management (TCM) framework includes:
- Real-time ADT (Admit, Discharge, Transfer) alerts
- Patient contact within 48 hours
- Medication reconciliation
- Care plan review
- Scheduled follow-up within 7–14 days
- Documentation of all interactions
When these steps are tracked and standardized, patients are less likely to destabilize unnoticed.
Beyond clinical benefits, compliant TCM programs may also allow facilities and aligned providers to capture appropriate reimbursement under CMS guidelines when eligibility criteria are met.
2. Prioritize Medication Reconciliation Within 48 Hours
Medication discrepancies are one of the most common causes of rehospitalization.
High-performing SNFs:
- Review discharge instructions line-by-line
- Verify new prescriptions and discontinued drugs
- Confirm dosing accuracy
- Educate patients and caregivers
- Document reconciliation clearly
This simple process significantly lowers avoidable transfers due to adverse drug events.
3. Use Remote Patient Monitoring (RPM) for High-Risk Residents
Many readmissions are preceded by subtle physiological warning signs:
- Weight gain in heart failure
- Rising blood pressure
- Oxygen desaturation in COPD
- Glucose instability in diabetic patients
Remote Patient Monitoring (RPM) enables real-time tracking of these indicators, allowing staff to intervene early.
For eligible Medicare populations, RPM may be billed in compliance with CMS requirements when implemented correctly. More importantly, it shifts care from reactive to proactive — reducing emergency transfers.
4. Strengthen Chronic Care Management (CCM)
Residents with two or more chronic conditions require continuous oversight.
Chronic Care Management programs provide:
- Monthly non-face-to-face care coordination
- Ongoing medication adherence support
- Personalized care plans
- Regular check-ins
When consistently delivered, CCM reduces complications that often lead to hospitalization.
Economically, structured CCM programs can create recurring revenue streams while stabilizing patient outcomes, a rare combination of financial and clinical upside.
5. Standardize Early Warning Protocols
Top-performing SNFs establish defined escalation thresholds, such as:
- Rapid weight changes
- Elevated systolic blood pressure
- Reduced oxygen saturation
- Changes in cognitive status
- Abnormal lab trends
Automated alerts and defined escalation pathways reduce decision delays.
Facilities that rely solely on manual tracking often miss subtle warning signs. Structured monitoring improves consistency across shifts and teams.
6. Integrate Social Determinants of Health (SDOH) Assessments
Transportation barriers, medication affordability, limited caregiver support, and food insecurity can all drive readmissions.
Incorporating SDOH screening into admission workflows enables proactive intervention.
Facilities that treat both medical and non-medical drivers of health demonstrate stronger long-term outcomes and improved quality metrics.
How Do These Actions Improve Ratings?
Reducing readmissions does more than prevent hospital transfers; it directly strengthens performance across multiple CMS quality dimensions.
Here’s how:
1. Improved Rehospitalization Metrics
Lower 30-day readmission rates positively influence the quality measures incorporated into the CMS Five-Star Rating System and SNF VBP scoring. Improved performance here can raise overall star ratings.
2. Better Care Transition Scores
Structured Transitional Care Management demonstrates reliable post-discharge coordination. Facilities that document timely follow-up, medication reconciliation, and communication show stronger performance in care transition measures.
3. Enhanced Clinical Stability
Proactive monitoring and chronic care coordination reduce acute exacerbations. More stable residents translate to fewer emergency transfers, better survey outcomes, and stronger quality indicators.
4. Stronger Documentation & Compliance
Standardized workflows improve documentation consistency — a critical factor during CMS surveys and audits. Facilities that can demonstrate clear, repeatable processes often perform better in regulatory reviews.
5. Improved Referral Reputation
Hospitals track post-acute outcomes closely. When an SNF consistently demonstrates lower readmission rates, discharge planners are more likely to prioritize that facility, thereby strengthening referral pipelines.
In short, structured care coordination improves both measured outcomes and perceived performance, the two drivers of ratings and reputation.
Connecting Readmission Reduction to Economic Performance
For SNF leaders focused on margins, here’s how these strategies translate financially:
Higher Ratings → Stronger Referral Volume
Improved star ratings influence hospital discharge decisions and family choice.
Reduced VBP Risk
Fewer readmissions minimize negative payment adjustments.
Expanded Reimbursable Services
Structured TCM, CCM, and RPM programs — when implemented compliantly — create additional revenue pathways.
Lower Operational Disruption
Preventing unnecessary hospital transfers reduces administrative burden and transportation costs.
The economic impact compounds over time as referral relationships strengthen.
The Implementation Challenge for SNFs
While the strategies above are clear, many SNFs face real operational constraints:
- Nursing shortages
- Limited care coordination staff
- Documentation burden
- Compliance anxiety
- Technology fragmentation
Executing a comprehensive readmission reduction model requires both infrastructure and staffing consistency — two areas that are often stretched thin.
Scaling Readmission Reduction Without Adding Staff
This is where many SNFs look for operational partners.
Circle Health Care supports Skilled Nursing Facilities by implementing structured:
- Transitional Care Management workflows
- Chronic Care Management programs
- Remote Patient Monitoring
- Dedicated clinical staffing support
Our model combines AI-powered technology with NCLEX-certified RNs and licensed clinical teams who act as an extension of the facility.
For SNFs, this means:
- No upfront technology investment
- No new hires required
- Automated compliance tracking
- Real-time documentation visibility
- Consolidated billing summaries
The result is a coordinated, scalable infrastructure for readmission reduction that aligns clinical outcomes with financial performance.
For facilities evaluating how to operationalize these strategies, exploring a structured care management model can be a practical next step.
Conclusions Readmission Reduction Is a Competitive Advantage
In today’s value-based landscape, reducing readmissions is no longer optional.
For SNFs, it directly impacts:
- Star ratings
- Medicare reimbursement
- Referral pipelines
- Market reputation
- Financial stability
Facilities that implement structured transitional workflows, proactive monitoring, and coordinated chronic care programs consistently outperform peers.
The difference is not intent — it is execution.
SNFs that treat readmission reduction as an integrated operational strategy, rather than a reactive compliance task, position themselves for sustainable growth in a value-driven healthcare environment.
Ready to Strengthen Your SNF’s Readmission Strategy?
If your facility is evaluating how to reduce 30-day rehospitalizations, protect ratings, and improve financial performance without expanding staff, speak with a care management expert to explore how structured transitional care management, chronic care management, and remote patient monitoring programmes can support your goals.
Schedule a demo to see how Circle Care can support your SNF with structured care coordination and comprehensive care management solutions designed to improve outcomes and strengthen transitions.
Frequently Asked Questions
1. How do readmissions affect SNF star ratings?
A. CMS incorporates rehospitalization measures into the Five-Star Quality Rating System, which influences referral volume and public perception.
2. Can SNFs participate in Transitional Care Management?
A. When eligibility criteria are met and documentation standards are followed, TCM services may be billed under CMS guidelines. Always verify current requirements and consult your billing team.
3. Is Remote Patient Monitoring appropriate in an SNF setting?
A. RPM may be appropriate for eligible residents with chronic conditions requiring ongoing physiological monitoring. Implementation must follow CMS documentation and supervision requirements.
4. How quickly can readmission rates improve?
A. Facilities implementing structured transitional workflows and proactive monitoring often see measurable improvements within 6–12 months.
5. How can SNFs measure whether their readmission reduction strategy is working?
A. SNFs should track 30-day hospital readmission rates, CMS rehospitalization quality measures, and SNF value-based purchasing performance reports. Monitoring trends monthly, alongside internal metrics such as medication reconciliation completion and timely post-discharge follow-up, helps facilities identify gaps early and demonstrate measurable improvement over time.
Clinical Guidance Disclaimer: This content is intended for general informational purposes only and does not constitute medical or clinical advice. Care management programs should be implemented under the supervision of qualified healthcare professionals in compliance with applicable regulations.