

Learn the CMS TEAM Model for hospitals improve post-acute coordination, reduce readmissions, and enhance patient outcomes with this practical guide.
Today’s healthcare leaders face increasing pressure to coordinate care across settings, not just inside the hospital. To accelerate value-based transformation, the Centers for Medicare & Medicaid Services (CMS) is launching a new mandatory model that shifts accountability for patient outcomes, costs, and transitions well beyond discharge.
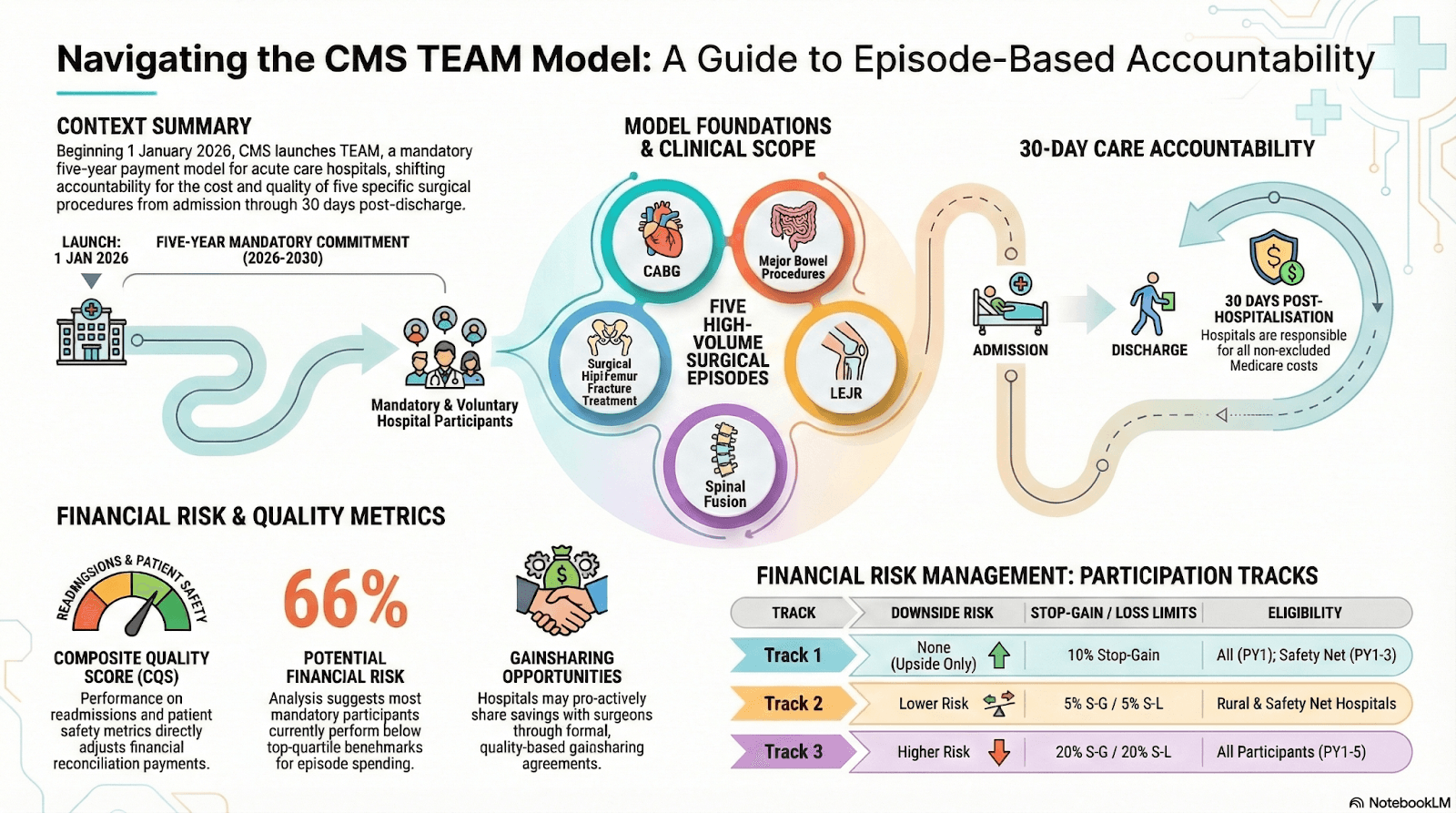
The Transforming Episode Accountability Model (TEAM) represents a fundamental evolution in federal policy: hospitals will be accountable not only for inpatient care but for the entire surgical episode, including the critical 30-day window that follows discharge.
This playbook-style guide explains what TEAM is, why it matters, how it works, and how hospitals, health systems, and post-acute care partners, including skilled nursing facilities (SNFs), must prepare to succeed.
What Is the CMS TEAM Model?
The Transforming Episode Accountability Model (TEAM) is a mandatory bundled payment initiative beginning January 1, 2026 for selected acute care hospitals in designated Core-Based Statistical Areas (CBSAs).
Under TEAM:
- Hospitals are held accountable for total cost and quality of care from surgery through 30 days post-discharge.
- The model applies to Medicare Part A & B beneficiaries undergoing one of five high-impact procedures:
- Lower extremity joint replacement
- Surgical hip and femur fracture treatment
- Spinal fusion
- Coronary artery bypass graft (CABG)
- Major bowel procedures
This accountability includes services provided in hospitals and post-acute settings such as SNFs, rehabilitation, outpatient therapy, and follow-up care.
Unlike traditional fee-for-service, where hospitals are paid for discrete visits or stays, TEAM ties payments and financial performance to the entire episode, pushing providers toward integrated, coordinated care delivery.
Why TEAM Matters for Hospitals and Health Systems?
From Volume to Value
TEAM shifts responsibility:
- From isolated inpatient care
- To whole-episode outcomes, incentivizing continuity and seamless transitions. Hospitals are evaluated not just on procedural success but on the quality and cost of recovery.
Reduced Hospitalizations
By making hospitals accountable for readmissions and ED visits within 30 days of discharge, TEAM encourages proactive care planning and follow-up engagement across care settings.
Quality and Cost Alignment
Financial results are tied to both quality performance and total spending:
- Performing below the target cost can yield reconciliation bonuses
- Exceeding the target cost or lower quality can result in penalties or reduced shared savings
This alignment promotes long-term clinical quality and cost efficiency, core goals of value-based care.
Financial and Quality Implications Under TEAM
TEAM introduces meaningful financial risk, and opportunity, depending on how well hospitals manage episode cost and quality performance.
Financial Risk: Episode Cost Overruns
Hospitals are assigned a target price per episode. If actual spending exceeds that benchmark, the hospital may owe Medicare the difference.
Even small variances can escalate quickly.
Example:
If a hospital averages $2,000 above the CMS target price across 200 surgical episodes, that results in a $400,000 repayment obligation. Multiply that across multiple procedure categories, and exposure increases significantly.
This makes cost control across post-acute settings essential; not optional.
Readmissions: A Double Impact
Thirty-day readmissions affect TEAM performance in two ways:
- Increase total episode spending
- Lower the Composite Quality Score (CQS)
Because reconciliation payments are adjusted based on quality performance, higher readmission rates can:
- Reduce or eliminate potential bonus payments
- Increase downside repayment exposure
- Lower overall financial performance under the model.
Quality Score Influence on Payment
The Composite Quality Score (CQS) directly influences how much of any reconciliation payment a hospital can retain.
Strong quality performance:
- Protects shared savings
- Enhances bonus potential
Weak quality performance:
- Reduces reconciliation gains
- Amplifies financial penalties.
Why Post-Acute Network Performance Matters?
Since much of the 30-day episode occurs outside the hospital, performance of SNFs, home health agencies, and rehabilitation providers directly affects:
- Readmission rates
- Length of stay
- Total episode cost
- Quality scoring
Hospitals must evaluate historical performance data and continuously monitor network outcomes during TEAM performance years.
Under TEAM, post-acute coordination is no longer a discharge planning function, it is a financial strategy.
Key Requirements in the TEAM Model
Participating hospitals will need to demonstrate capability across these core areas:
1. Seamless Care Coordination
Hospitals must coordinate care from surgery through post-acute settings, including rehabilitation, home health, and SNFs. Fragmented transitions lead to complications, readmissions, and cost overruns, all of which TEAM seeks to reduce.
2. Post-Acute Visibility
Hospitals must eliminate the “post-acute black hole” — the lack of real-time visibility into what happens after discharge. Strong analytics, data sharing, and predictive insights are essential to track patient progress, identify risk early, and intervene before complications occur.
3. Primary Care Engagement
TEAM emphasizes continuity beyond post-acute care: hospitals are expected to support referrals and connections to primary care to improve long-term outcomes.
4. Quality Performance
Quality measures related to readmission rates, patient safety composites, and patient-reported outcomes influence reconciliation results. Hospitals must perform well not just clinically but across integrated quality benchmarks.
5. Data and Technology
Success under TEAM depends on interoperable systems that share clinical data across settings, allowing timely alerts and confirming information exchange. Integrated platforms help reduce gaps and ensure accurate claims and reconciliation data.
Preparing for TEAM: Strategic Priorities
To succeed, hospitals and health systems need a proactive strategy that includes:
Post-Acute Care Visibility
Actively monitor patient status in real time across all post-acute settings. Predictive analytics and interoperable health IT solutions convert hidden risk into actionable intervention opportunities.
Stronger Partnerships with SNFs and PAC Providers
Collaborative relationships with SNFs, home health agencies, and rehabilitation facilities ensure a shared understanding of care expectations and measurable quality outcomes. Working with high-performing partners can reduce episode costs and improve outcomes.
Technology-Enabled Communication
Coordinated care requires systems that enable secure, instantaneous exchange of clinical and administrative data among hospitals, PAC providers, primary care, and analytics teams.
Standardized Discharge Workflows
Consistent discharge planning and handoff procedures eliminate miscommunication and prevent care delays, a critical factor in reducing avoidable readmissions.
Data-Driven Quality Improvement
Use episode-level data to identify patterns, intervene early, and refine processes. Hospitals that can demonstrate data-backed improvements are better positioned for reconciliation bonuses.
Implications for SNFs and Post-Acute Care Partners
TEAM reshapes how hospitals view SNFs and other post-acute providers:
- SNFs with strong performance and low readmission rates become strategic partners under TEAM.
- Quality and cost outcomes in post-acute care directly influence a hospital’s TEAM performance.
- Hospitals may increasingly align preferred networks based on performance data and shared accountability.
This creates incentives for SNFs to adopt standardized care processes, improve communication workflows, and participate in integrated data systems.
Expected Outcomes Under TEAM
The TEAM model aims to achieve:
- Reduced avoidable readmissions
- Shorter recovery times
- Lower total episode costs
- Stronger alignment across care settings
- Enhanced patient experience
- Better long-term outcomes through primary care linkage.
These results require investments in care coordination infrastructure, analytics, and partnership frameworks.
Conclusion: TEAM as a Value-Based Catalyst
The CMS TEAM Model represents one of the most significant shifts in Medicare payment strategy in recent years. By holding hospitals accountable for entire episodes, from surgery through 30 days after discharge — TEAM pushes care coordination and quality improvement front and center.
To succeed, organizations must build technology-enabled, data-driven, partnership-oriented approaches to post-acute care, turning fragmented handoffs into seamless continuums of care.
For SNFs and health systems alike, early strategic alignment with TEAM requirements is not just compliance, it’s a competitive advantage in a value-based future.
Frequently Asked Questions
1. When does TEAM take effect?
The mandatory phase begins January 1, 2026, and will run through December 31, 2030.
2. Which hospitals are required to participate?
Hospitals located in selected Core-Based Statistical Areas (CBSAs) are mandated to participate, with criteria ending prior to voluntary bundled payment models.
3. What procedures does TEAM cover?
TEAM includes coronary artery bypass graft, joint replacement, spinal fusion, surgical hip and femur fracture treatment, and major bowel procedures.
4. Can hospitals choose their post-acute partners?
Yes. Hospitals can design preferred PAC networks based on performance, cost, and quality, creating opportunities for SNFs that demonstrate strong outcomes.
5. How does quality affect payment?
Quality performance influences reconciliation results — high performers may receive bonuses, while lower performers may see reduced reconciliation gains or penalties.