
Learn how Chronic Care Management (CCM) works, including CMS billing codes, compliance rules, workflows, and measurable outcomes for SNFs and physician groups.
Chronic conditions account for nearly 90% of healthcare spending in the United States. For Skilled Nursing Facilities (SNFs) and physician groups, managing patients with multiple chronic diseases is no longer episodic; it requires structured, ongoing coordination beyond office visits.
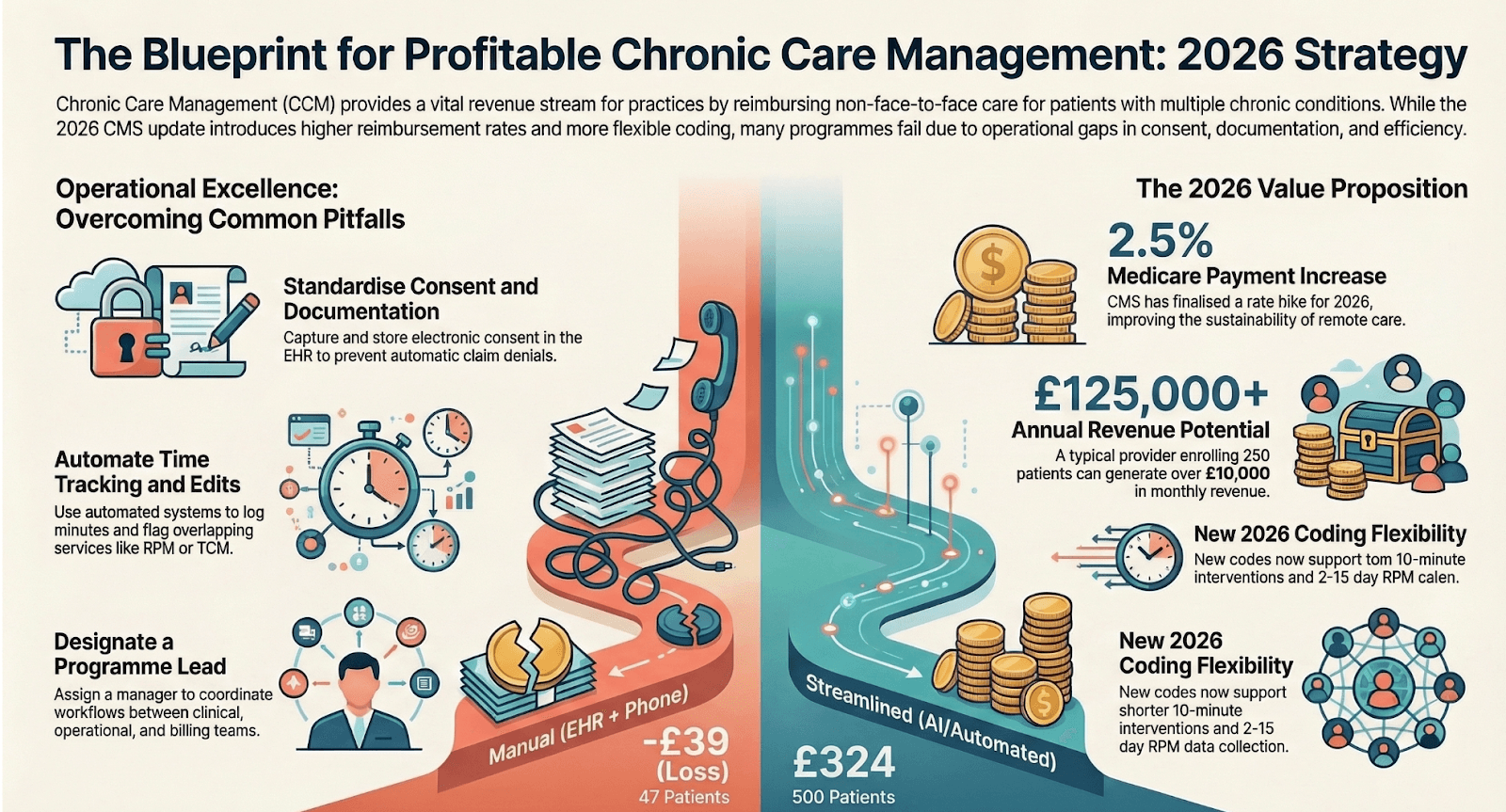
Chronic Care Management (CCM) was introduced by CMS to reimburse providers for non-face-to-face care coordination services delivered between appointments. But CCM is more than a billing opportunity. When operationalized correctly, it becomes infrastructure for reducing hospitalizations, improving quality performance, and supporting value-based reimbursement.
This guide explains CCM definitions, CMS billing codes, compliance requirements, workflow execution, financial implications, and measurable outcomes.
What Is Chronic Care Management (CCM)?
Chronic Care Management refers to structured care coordination services provided to Medicare beneficiaries with two or more chronic conditions expected to last at least 12 months (or until death) and that place the patient at significant risk of:
- Hospitalization
- Acute exacerbation
- Functional decline
- Death
CCM services occur outside face-to-face visits and include:
- Development and maintenance of a comprehensive electronic care plan
- Medication reconciliation and adherence monitoring
- Monthly patient outreach
- Coordination across providers and settings
- Preventive risk monitoring
For physician groups, CCM extends care longitudinally.
For SNFs, CCM is especially relevant during transitions from facility to community settings, ensuring continuity after discharge.
CMS CCM Billing Codes Explained
Understanding billing mechanics is critical for compliance and sustainability.
CPT 99490 – Standard CCM
- Minimum 20 minutes of clinical staff time per calendar month
- Directed by a physician or qualified healthcare professional
- Moderate to high complexity medical decision-making
- Requires comprehensive care plan documentation
CPT 99439 – Add-On Code
- Each additional 20 minutes of clinical staff time
- Billed in conjunction with 99490
CPT 99487 – Complex CCM
- Minimum 60 minutes of clinical staff time
- High-complexity medical decision-making
- Establishment or substantial revision of care plan
CPT 99489 – Complex Add-On
- Each additional 30 minutes beyond the initial 60 minutes
CPT 99491 – Physician/Qualified Provider Time
- At least 30 minutes personally delivered by the billing provider
Key Compliance Requirements
CMS requires:
- Documented patient consent (verbal or written)
- 24/7 access to care management support
- Electronic care plan accessible to the care team
- Accurate time tracking and activity logs
- Only one practitioner bills CCM per patient per month
Failure points often include insufficient documentation, unclear time aggregation, or duplicate billing across providers.
How CCM Works in Practice: End-to-End Workflow
Effective CCM is cyclical and structured.
1. Patient Identification & Risk Stratification
Organizations use EHR data, diagnosis codes, and utilization patterns to identify eligible patients. Risk stratification prioritizes those with high hospitalization probability.
2. Enrollment & Consent
Consent is documented, and patients are educated about monthly services and potential cost-sharing obligations.
3. Comprehensive Care Plan Creation
The care plan includes:
- Diagnoses
- Measurable health goals
- Medication list
- Specialist involvement
- Community resource coordination
- Social determinants considerations
This care plan must be electronically accessible and regularly updated.
4. Monthly Outreach & Monitoring
Clinical staff conducts structured outreach covering:
- Symptom progression
- Medication adherence
- Appointment compliance
- Emerging risks
- Social or functional barriers
5. Time Documentation & Billing
Time spent coordinating care is logged. Once minimum thresholds are met, billing is submitted under the appropriate CPT code.
6. Continuous Escalation Pathways
If worsening symptoms are identified, escalation occurs before conditions require emergency care.
For SNFs transitioning residents to outpatient management, CCM bridges discharge gaps, reducing fragmentation between facility and community providers.
Financial Impact of CCM
CCM generates recurring monthly reimbursement, but sustainability depends on operational efficiency.
Key variables include:
- Percentage of eligible Medicare patients enrolled
- Average monthly engagement time
- Staffing model (in-house vs outsourced)
- Documentation accuracy
- Patient retention rates
For example, enrolling 100 eligible Medicare patients under CPT 99490 can create predictable recurring revenue streams. However, under-enrollment or inconsistent outreach reduces margin potential.
Operational costs must also be considered:
- Care coordinator salaries
- Technology systems
- Compliance oversight
- Reporting infrastructure
When executed efficiently, CCM supports both revenue stability and downstream cost avoidance through reduced hospitalizations.
Outcomes of Structured CCM Programs
When Chronic Care Management is implemented as a structured, data-driven programme, not just a billing exercise, it produces measurable clinical, financial, and operational outcomes. The impact extends beyond monthly reimbursement and directly influences total cost of care, utilization trends, and quality performance metrics.
1. Reduction in Avoidable Hospitalizations and ED Visits
Regular monthly outreach enables early detection of symptom escalation, medication side effects, or non-adherence before they result in acute events. Patients with CHF, COPD, and diabetes benefit especially from proactive monitoring.
Structured CCM programs have been associated with:
- Lower 30-day readmission rates
- Reduced emergency department utilization
- Fewer exacerbation-driven admissions
- Earlier intervention in high-risk patients
For SNFs transitioning residents back into the community, CCM acts as a safety net during the highest-risk post-discharge window.
2. Improved Chronic Disease Control
Ongoing medication reconciliation, lifestyle reinforcement, and goal tracking improve measurable health indicators over time.
Common improvements include:
- Better HbA1c control in diabetic populations
- Stabilized blood pressure in hypertensive patients
- Reduced COPD flare-ups
- Improved CHF symptom management
This longitudinal engagement helps shift care from reactive crisis management to proactive stabilization.
3. Enhanced Medication Adherence and Safety
Polypharmacy is a major driver of hospitalizations among Medicare populations. Monthly CCM touchpoints reduce confusion around dosage changes, refill gaps, and drug interactions.
Programs consistently report:
- Fewer adverse drug events
- Higher medication refill compliance
- Improved understanding of treatment plans
- Reduced duplicative prescriptions across providers
For physician groups managing complex panels, this strengthens overall medication oversight.
4. Stronger Value-Based Performance Metrics
CCM supports performance in alternative payment models by directly influencing metrics tied to chronic disease management and utilization control.
It contributes to:
- MIPS quality scores
- ACO shared savings performance
- HEDIS chronic disease measures
- Total cost of care reduction targets
- Star rating components in applicable programs
Because value-based contracts increasingly reward prevention over volume, CCM becomes a structural lever for performance improvement.
5. Predictable, Recurring Reimbursement
Unlike episodic billing tied to office visits, CCM generates monthly recurring revenue aligned with care coordination activities. When enrollment and documentation are consistent, this creates financial predictability.
Operationally mature CCM programs demonstrate:
- Stable monthly reimbursement streams
- Improved revenue per Medicare beneficiary
- Better alignment between clinical effort and financial return
For physician groups, this diversifies revenue beyond visit-based billing. For SNFs collaborating with affiliated physicians, it strengthens post-discharge continuity and shared performance incentives.
6. Increased Patient Engagement and Retention
Patients enrolled in CCM programs report feeling supported between visits. Regular touchpoints foster stronger provider relationships and increase adherence to follow-up appointments.
Organizations often observe:
- Higher patient satisfaction scores
- Reduced care fragmentation
- Greater continuity with primary providers
- Improved long-term patient retention
In competitive healthcare markets, this continuity enhances both clinical stability and organizational reputation.
7. Organizational Learning and Data Visibility
Structured CCM programs generate longitudinal data about symptom trends, utilization triggers, and care coordination gaps. Over time, this data supports better risk stratification and targeted interventions.
Mature programs leverage CCM data to:
- Identify high-risk cohorts earlier
- Refine outreach prioritization
- Improve discharge planning
- Strengthen population health strategies
This creates compounding operational intelligence beyond immediate billing impact.
Common Implementation Pitfalls
Despite its structure, many CCM programs struggle due to:
- Manual documentation burdens
- Staff bandwidth limitations
- Inconsistent patient outreach
- Fragmented knowledge systems
- Lack of standardized workflows
- Poor time tracking accuracy
These gaps create compliance risks and erode financial viability.
How Organizations Scale CCM Efficiently
To scale CCM without overwhelming internal teams, organizations require:
- Dedicated care coordination staff
- Automated documentation prompts
- Centralized care plan templates
- Standardized outreach scripts
- Integrated time tracking systems
- Performance dashboards
Many physician groups and SNFs choose to build internal infrastructure. Others partner with specialized care management providers to ensure compliance, standardize workflows, and reduce administrative load.
For example, Circle Health Care supports physician organizations and post-acute networks with structured CCM workflows, AI-enabled documentation systems, and dedicated clinical teams that help maintain CMS compliance while streamlining monthly engagement cycles. This type of model allows organizations to implement CCM without expanding internal operational complexity.
CCM Within Value-Based Care Strategy
CCM is foundational to value-based care participation.
It strengthens:
- Accountable Care Organizations (ACOs)
- Risk-based contracts
- Population health programs
- Total cost of care management
As reimbursement models shift toward outcomes rather than volume, longitudinal care coordination becomes a strategic requirement, not just a billing option.
The Bottom Line
Chronic Care Management transforms episodic care into continuous coordination. For SNFs and physician groups, it provides a structured pathway to improve patient outcomes, support value-based performance, and create sustainable reimbursement aligned with proactive care delivery.
Organizations that approach CCM as an operational system, rather than simply a billing code, are better positioned to reduce hospital utilization, strengthen continuity, and build scalable care coordination infrastructure for the future.
Frequently Asked Questions
1. Can SNFs bill CCM directly?
Typically, CCM is billed by the physician or qualified billing provider managing outpatient care. SNFs may support coordination, but must align with CMS billing rules.
2. How much revenue can CCM generate?
Revenue depends on enrollment size, code utilization, and documentation consistency. Predictable monthly reimbursement is possible with structured execution.
3. Does CCM reduce hospital readmissions?
Yes. Proactive outreach and medication management reduce preventable exacerbations and ED visits.
4. Is patient consent required?
Yes. Documented consent is mandatory before billing.
5. How is CCM different from RPM or TCM?
CCM focuses on ongoing chronic disease management. RPM centers on device-based physiologic monitoring. TCM addresses post-discharge transitions for limited timeframes.